US FDA grants breakthrough therapy designation to Boehringer Ingelheim’s volasertib to treat patients with AML « New Drug Approvals:
'via Blog this'
Friday, 20 September 2013
Thursday, 19 September 2013
Tuesday, 17 September 2013
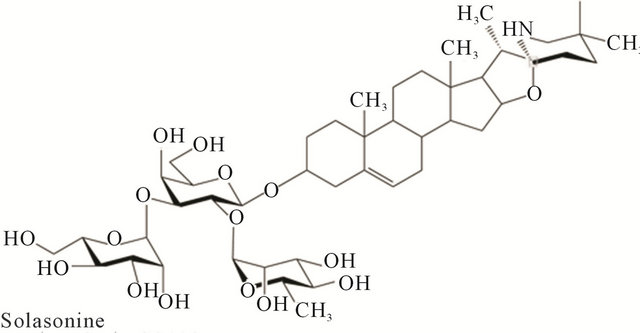
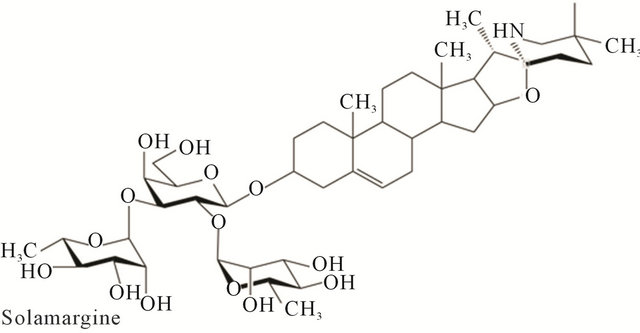
Drug therapy: Solamargine and other solasodine rhamnosyl glycosides as anticancer agents
Modern ChemotherapyVol.2 No.2(2013), Article ID:30489,17 pagesDOI:10.4236/mc.2013.22005
Drug therapy: Solamargine and other solasodine rhamnosyl glycosides as anticancer agents
Australasian Institute of Medical Research, Brisbane, Australia; bill.cham@gmail.com
Copyright © 2013 Bill E. Cham. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 24 February 2013; revised 26 March 2013; accepted 5 April 2013
Keywords: Cancer; Skin Cancer; Solamargine; Solasonine; BEC; Solasodine Rhamnosyl Glycosides; CuradermBEC5; Apoptosis; Antineoplastic; Targeted Therapy
ABSTRACT
In the last century, the discovery of cytotoxic agents was revolutionary for anticancer therapy. These therapies have resulted in better understanding of cancer in general. However, the development of agents that combine efficacy, safety and convenience remains a great challenge. The narrow, if not adverse, therapeutic index of most drugs, the damage not only to cancer cells, but also to normal and healthy tissue and the occurrence of resistance have limited anticancer efficacy. This review presents the development of promising novel cytotoxic solasodine rhamnosyl glycoside drugs that offer not only gains in specificity and efficacy, but also in safety, tolerability, non-resistance and convenience in the treatment of patients with cancer.
1. INTRODUCTION
In the past 100 years our understanding of the biology of cancer has come a long way. We now have a reasonable working knowledge of how tumors initially form, grow and spread. Importantly, substantial information about features distinguishing tumor from normal cells is being accumulated, resulting in major new insights into cancer biology................
read all at
Scripps Research Institute Scientists Create Extremely Potent and Improved New Derivatives of Successful Anticancer Drug

Dale Boger, PhD, is chair of the Department of Chemistry at The Scripps Research Institute.
LA JOLLA, CA—September 16, 2013—Scientists at The Scripps Research Institute (TSRI) have found a way to make dramatic improvements to the cancer cell-killing power of vinblastine, one of the most successful chemotherapy drugs of the past few decades. The team’s modified versions of vinblastine showed 10 to 200 times greater potency than the clinical drug. Even more significantly, these new compounds overcome the drug resistance that emerges upon treatment relapse, which renders continued or subsequent vinblastine treatment ineffective in some patients.
The TSRI researchers expect that similar modifications will boost the effectiveness of vincristine, a closely related drug that is commonly used against childhood leukemias and Hodgkin’s disease.
http://www.scripps.edu/news/press/2013/20130916boger.html
vincristine

http://www.scripps.edu/news/press/2013/20130916boger.html

vincristine
Sunday, 15 September 2013
LEVOCETRIZINE

LEVOCETRIZINE
Levocetirizine (as levocetirizine dihydrochloride) is a third-generation non-sedative antihistamine, developed from the second-generation antihistamine cetirizine. Chemically, levocetirizine is the active enantiomer of cetirizine. It is the R-enantiomer of the cetirizine racemate. Levocetirizine works by blocking histamine receptors. It does not prevent the actual release of histamine from mast cells, but prevents it binding to its receptors. This in turn prevents the release of other allergy chemicals and increased blood supply to the area, and provides relief from the typical symptoms of hay fever.
The manufacturers claim it to be more effective with fewer side effects than the second-generation drugs; however, there have been no published studies supporting this assertion, although other studies have concluded it may be more effective.[1]
History and formulations
Levocetirizine was first launched in 2001 by Belgian pharmaceutical company UCB. It is sold under the brand name Xyzal/ˈzaɪzæl/ in Australia, Czech Republic, Austria, Finland, France, Ireland, Netherlands, Portugal, Romania, Taiwan, Turkey, United States, South Africa and UK; Xuzal in Mexico; Xusal in Germany; and Xozal in Greece. In Hungary it is marketed by Richter Gedeon under the Zilola brand name.
In India, levocetirizine is marketed by GlaxoSmithKline under the brand name Vozet and Xyzal. On May 25, 2007, theUnited States Food and Drug Administration approved Xyzal, where it is co-marketed by Sanofi-Aventis. Torrent Pharma launched UVNIL in rural market of India. It is also available as LEZYNCET 5 mg tablets through Unichem in India. In India, generic name of Lev-Cit 5 mg is manufactured by VIP Pharmaceuticals. Also marketed in India by Croslands (Ranbaxy Laboratories Ltd.) under the brand name Teczine. In Brazil it is marketed under the brand name 'Zyxem' by Farmalab. It is marketed in Egypt by BORG Pharma under the brand name 'Xaltec', Allear by western pharmaceuticals and levcet by marcryl.
In Pakistan levocetirizine was first launched in liquid formulation by Novartis Consumer Health Division by the name of T-Day Syrup. It is available as 5 mg-strength tablets and a 0.5 mg/mL oral solution. In Pakistan levocetirizine is available in liquid formulation as well with the name of OCITRA and T-Day 2.5 mg/5 mL. In Bangladesh levocetirizine is available in 5 mg tablet & 2.5 mg/5 mL oral liquid formulation with the brand name of Alcet marketed by Healthcare Pharmaceuticals and Seasonix marketed by Incepta Pharmaceuticals. In Nepal levocetirizine is available in 5 mg tablet with brand name ofCurin manufactured by Beximco Pharma.[2]
Side effectsl
levocetirizine is called a non-sedating antihistamine as it does not enter the brain in significant amounts, and is therefore unlikely to cause drowsiness. However, some people may experience some slight sleepiness, headache, mouth dryness,lightheadedness, vision problems (mainly blurred vision), palpitations and fatigue.[3]
Research
latest research shows levocetirizine reduces asthma attacks by 70% in children.[4]
Availability
The drug is currently available by prescription in the United States. Although the drug was only authorized by the FDA on 25 May 2007, it was already available in most European countries. Like many new drugs it entered the market at a higher price than currently available third and second generation antihistamines. In India, one form of the drug is available as Crohist MK tablets and syrup, a formulation of levocetirizine hydrochloride and montelukast. In India, Crohist MK is a Schedule 'H' drug and may only be prescribed by a registered medical practitioner. In Finland, the drug is sold over-the-counter.

- ^ Grant, JA; Riethuisen, JM; Moulaert, B; DeVos, C; Gamalero, C.; Descalzi, D.; Folli, C.; Passalacqua, G. et al. (2002-02). "A double-blind, randomized, single-dose, crossover comparison of levocetirizine with ebastine, fexofenadine, loratadine, mizolastine, and placebo: suppression of histamine-induced wheal-and-flare response during 24 hours in healthy male subjects.". Ann Allergy Asthma Immunol 88 (2): 190–197. doi:10.1016/S1081-1206(10)61995-3. PMID 11868924.
- ^ http://www.beximco-pharma.com/allergic-disorders/147-curin.html
- ^ XOZAL technical specifications booklet.
- ^ Pasquali, M; Baiardini, I; Rogkakou, A; Riccio, AM; Gamalero, C; Descalzi, D; Folli, C; Passalacqua, G et al. (2006-09)."Levocetirizine in persistent allergic rhinitis and asthma: effects on symptoms, quality of life and inflammatory parameters.".Clinical & Experimental Allergy 36 (9): 1161–7. doi:10.1111/j.1365-2222.2006.02548.x. PMID 16961716.

Figure 1-The chemical structure of Xyzal
Cetirizine, chemically [2-[4-[(4-chlorophenyl)phenylmethyl]-1-piperazinyl]ethoxy]acetic acid is an antihistamine non-sedating type histamine H1-receptor antagonist, indicated for relief of symptoms associated with seasonal allergic rhinitis, perennial allergic rhinitis and related diseases.
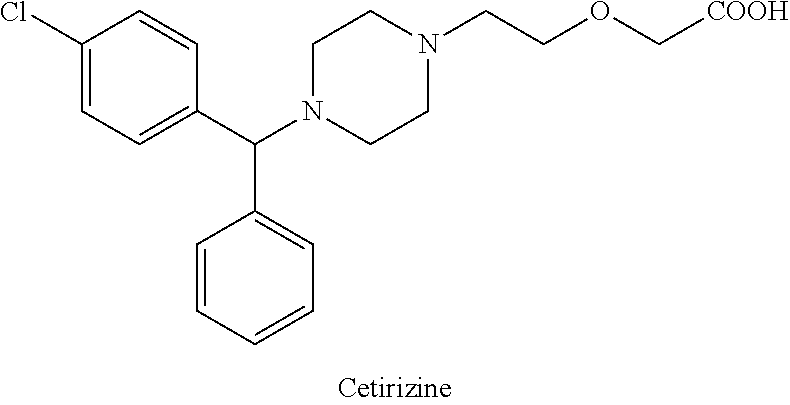
U.S. Pat. No. 4,525,358 and its equivalent EP 58146 disclose cetirizine and its pharmaceutically acceptable salts. The process for the synthesis of cetirizine comprises condensation of 1-[(4-chlorophenyl)-phenylmethyl]piperazine with 2-chloroethoxy acetamide to obtain 2-[2-[4-[(4-chlorophenyl)phenylmethyl]-1-piperazinyl]-ethoxy acetamide which on hydrolysis gives cetirizine.
It was found later that the pharmacological activity resides primarily in (R)-isomer or (−) form known as levocetirizine. GB 2225321 describes a process for the preparation of the dextro and levorotatory isomers of cetirizine comprising hydrolysis of 2-[2-[4-[(4-chlorophenyl)phenylmethyl]-1-piperazynyl]-ethoxy acetonitrile.

(−)-1-[(4-chlorophenyl)-phenylmethyl]piperazine is a very important intermediate in the synthesis of levocetirizine. U.S. Pat. No. 5,478,941 discloses a process for the synthesis of (−)-1-[(4-chlorophenyl)-phenylmethyl]piperazine involving hydrolyzing 1-[(4-chlorophenyl)-phenylmethyl]-4-(4-methylphenyl)sulfonyl piperazine with hydrobromic acid in the presence of 4-hydroxybenzoic acid.
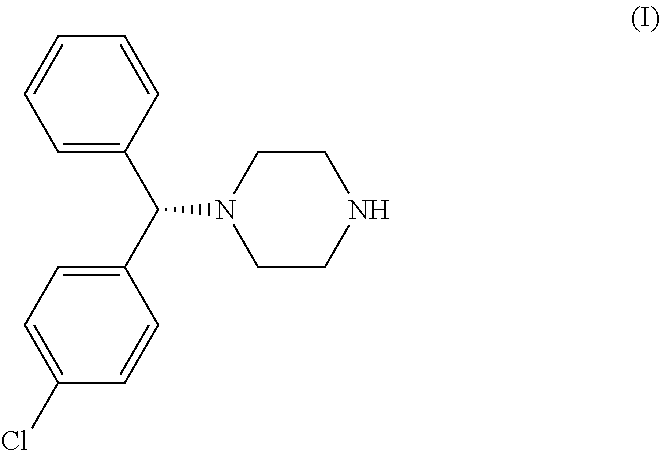
The alternative routes of synthesis of (−)-1-[(4-chlorophenyl)-phenylmethyl]piperazine disclosed in the prior art involve the use of bis chloro ethylamine which is carcinogenic in nature.
Levocetirizine is a highly-potent non-sedating anti-allergic agent. Hence, there are continuous attempts to develop new processes for the synthesis of levocetirizine and its intermediates. The present invention describes a new process for the preparation of the key intermediate (−)-1-[(4-chlorophenyl)-phenylmethyl]piperazine.
Levorotatory [2-[4-[(4-chlorophenyl)phenylmethyl]-1-piperazinyl]ethoxy]acetic acid, also known by the generic name of levocetirizine, has proven useful as a therapeutic agent for the treatment of allergic disease.
Levocetirizine and its salts including its dihydrochloride are known and are effective in the treatment of allergies, including but not limited to, chronic and acute allergic rhinitis, allergic conjunctivitis, pruritus, urticaria and the like. Levocetirizine belongs to the second generation of H1 histamine receptor antagonists, which are believed to offer significant advantages over first generation compounds. Studies have shown that levocetirizine provides safe and effective symptomatic relief of seasonal allergies. Levocetirizine is used also for treating chronic idiopathic urticaria.
GB 2,225,321 describes a process for the preparation of cetirizine in the levorotatory form, dextrorotatory form or a mixture thereof comprising the hydrolysis of enantiomerically pure [2-[4-[(4-chlorophenyl)phenylmethyl]-1-piperazinyl]ethoxy]acetonitrile. Hydrolysis takes place in aqueous, alcoholic or aqueous-alcoholic medium by a base or by an acid; the acid thus obtained is converted to its dihydrochloride. Optically active starting material 1-[(4-chlorophenyl)phenylmethyl]piperazine is obtained by resolution of the corresponding racemic compound, preferably by conversion to its diastereoisomeric salt with tartaric acid. The yield of resolution is rather low, namely only 12.7%. The obtained optically active intermediate is further converted with chloroethoxyacetonitrile in 69% yield.
EP 0 617 028 and EP 0 955 295 disclose a process for the preparation of optically active 1-[(4-chlorophenyl)phenylmethyl]piperazine and its conversion to cetirizine in the levorotatory form or dextrorotatory form or to derivative thereof. The process for the preparation is shown in the following scheme:

The drawback of the disclosed reaction is that it requires protection of N,N-bis(2-haloethyl)amine, and consequently deprotection of the intermediate obtained.
Preparation of Cetirizine in its Levorotatory Form Proceeds in most known syntheses from enantiomerically pure 1-[(4-chlorophenyl)phenylmethyl]piperazine. Consequently it appears to be very desirable to provide new routes to prepare the enantiomers thereof with improved optical purity and good yields.
Polymorphic form I of crystalline levorotatory dihydrochloride salt of cetirizine and amorphous form thereof are disclosed in WO 2004/050647 and WO 2004/065360. Crystalline form is prepared by crystallization from ketone-containing solvent, such as acetone, methyl ethyl ketone, dimethylketone, 2-pentanone and mixtures thereof. Amorphous form was prepared by solvent evaporation.
There still exists a need for an efficient synthesis of levocetirizine, new intermediates used in the process, suitable for large-scale production.
Synthesis of Xyzal:
Figure 2 displays the synthesis of Cetirizine (Zyrtec). Levocetirizine, the R-enantiomer of cetirizine, is then formed from pyroglutamate salts in a synthesis that does not have attainable details.
The synthesis of Cetrizine begins by reducing molecule 33 with a catecholborane. This reaction yields molecule 34, which is then treated with tetraflouroboric acid and reacted with an amine, compound 35. In order to remove the chromium group, the compound is refluxed in pyridine and undergoes an acid hydrolysis. This results in a yield of cetrizine.
Identification of all chirality centers:
Stereogenic centers are carbon atoms that are bonded to 4 groups. Tetrahedral stereogenic centers are stereogenic centers that are not only bonded to 4 groups but are more importantly bonded to 4 different groups. If a molecule contains 1 tetrahedral stereogenic center it is said to be chiral (nonsuperimposable on its mirror image).If a given compound contains more than 1 stereogenic center it must be further analyzed to determine if it is chiral or achiral(superimosable on its mirror image). The carbon atom bonded to the phenyl groups was found to be a tetrahedral stereogenic center. Therefore,xyzal,which was found to contain only 1 tetrahedral stereogenic center is generally considered a chiral compound because it meets the requirements of chirality and does not have a plane of symmetry that superimposes one half of the molecule on the other and is not super imposable on its mirror image.
Spectral data for Xyzal (IR and NMR):


Figure 2 displays the synthesis of Cetirizine (Zyrtec). Levocetirizine, the R-enantiomer of cetirizine, is then formed from pyroglutamate salts in a synthesis that does not have attainable details.
 |
| (Figure 2) |
The synthesis of Cetrizine begins by reducing molecule 33 with a catecholborane. This reaction yields molecule 34, which is then treated with tetraflouroboric acid and reacted with an amine, compound 35. In order to remove the chromium group, the compound is refluxed in pyridine and undergoes an acid hydrolysis. This results in a yield of cetrizine.
Identification of all chirality centers:
Stereogenic centers are carbon atoms that are bonded to 4 groups. Tetrahedral stereogenic centers are stereogenic centers that are not only bonded to 4 groups but are more importantly bonded to 4 different groups. If a molecule contains 1 tetrahedral stereogenic center it is said to be chiral (nonsuperimposable on its mirror image).If a given compound contains more than 1 stereogenic center it must be further analyzed to determine if it is chiral or achiral(superimosable on its mirror image). The carbon atom bonded to the phenyl groups was found to be a tetrahedral stereogenic center. Therefore,xyzal,which was found to contain only 1 tetrahedral stereogenic center is generally considered a chiral compound because it meets the requirements of chirality and does not have a plane of symmetry that superimposes one half of the molecule on the other and is not super imposable on its mirror image.
Spectral data for Xyzal (IR and NMR):
ESCITALOPRAM

128196-01-0 ESCITALOPRAM
Escitalopram (also known under various trade names) is an antidepressant of the selective serotonin reuptake inhibitor (SSRI) class. It is approved by the U.S. Food and Drug Administration (FDA) for the treatment of adults and children over 12 years of age with major depressive disorder and generalized anxiety disorder. Escitalopram is the (S)-stereoisomer (enantiomer) of the earlier Lundbeck drug citalopram, hence the name escitalopram. Escitalopram is noted for its high selectivity with serotonin reuptake inhibition. The similarity between escitalopram and citalopram has led to accusations of “evergreening“, an accusation that Lundbeck has rejected.[1]
Escitalopram has FDA approval for the treatment of major depressive disorder and generalized anxiety disorder in adults.[2]
Off-label uses
Escitalopram is sometimes prescribed off-label for the treatment of other conditions: social anxiety disorder,[3] panic disorder[4]and obsessive-compulsive disorder.[5] There is some evidence favouring escitalopram over the antidepressants citalopram andfluoxetine in the first two weeks of major depression.[6] Concerns of sponsorship bias with the studies are however noted.[6] In another review escitalopram and sertraline had the highest rate of efficacy and acceptability among adults receiving treatment for major depression with second-generation antidepressants.[7]
Efficacy
There is some controversy over selective publishing of SSRI clinical trials.[8] A meta-analysis analyzing published as well as unpublished trials found placebos to be similarly effective to SSRIs in treating mild depression, although SSRIs were more effective than placebo in more severe cases, with the magnitude of SSRI superiority increasing with increasing depression severity.[9]
A series of randomized, double-blind trials have found Escitalopram to be more efficacious and have fewer adverse effects than Citalopram.[10][11][12][13] Meta-analysis show a “small” but statistically significant improvement in effect strength [14][15] and some dispute these findings.[16]
Pharmacology

Cipralex brand escitalopram 10mg package and tablet sheet
Escitalopram increases intrasynaptic levels of the neurotransmitter serotonin by blocking the reuptake of the neurotransmitter into the presynaptic neuron. Of the SSRIs currently on the market, escitalopram has the highest affinity for the human serotonin transporter (SERT). The enantiomer of escitalopram ((R)-citalopram) counteracts to a certain degree the serotonin-enhancing action of escitalopram. As a result, escitalopram has been claimed to be a more potent antidepressant than citalopram, which is a mixture of escitalopram and (R)-citalopram. In order to explain this phenomenon, researchers from Lundbeck proposed that escitalopram enhances its own binding via an additional interaction with another allosteric site on the transporter.[42] Further research by the same group showed that (R)-citalopram also enhances binding of escitalopram,[43] and therefore the allosteric interaction cannot explain the observed counteracting effect. In the most recent paper, however, the same authors again reversed their findings and reported that R-citalopram decreases binding of escitalopram to the transporter.[44] Although allosteric binding of escitalopram to the serotonin transporter is of unquestionable research interest, its clinical relevance is unclear since the binding of escitalopram to the allosteric site is at least 1000 times weaker than to the primary binding site.
In vitro studies using human liver microsomes indicated that CYP3A4 and CYP2C19 are the primary isozymes involved in the N-demethylation of escitalopram. The resulting metabolites, desmethylescitalopram and didesmethylescitalopram, are significantly less active and their contribution to the overall action of escitalopram is negligible.
History
Escitalopram was developed in close cooperation between Lundbeck and Forest Laboratories. Its development was initiated in the summer of 1997, and the resulting new drug application was submitted to the U.S. FDA in March 2001. The short time (3.5 years) it took to develop escitalopram can be attributed to the previous extensive experience of Lundbeck and Forest with citalopram, which has similar pharmacology.[45] The FDA issued the approval of escitalopram for major depression in August 2002 and for generalized anxiety disorder in December 2003. Escitalopram can be considered an example of “evergreening“[46] (also called “lifecycle management”[47])– the long-term strategy pharmaceutical companies use in order to extend the lifetime of a drug, in this case of the citalopram franchise. Escitalopram is an enantiopure compound of theracemic mixture citalopram, used for the same indication, and for that reason it required less investment and less time to develop. Two years after escitalopram’s launch, when the patent on citalopram expired, the escitalopram sales successfully made up for the loss. On May 23, 2006, the FDA approved a generic version of escitalopram by Teva.[48]On July 14 of that year, however, the U.S. District Court of Delaware decided in favor of Lundbeck regarding the patent infringement dispute and ruled the patent on escitalopram valid.[49]
In 2006 Forest Laboratories was granted an 828 day (2 years and 3 months) extension on its US patent for escitalopram.[50] This pushed the patent expiration date from December 7, 2009 to September 14, 2011. Together with the 6-month pediatric exclusivity, the final expiration date was March 14, 2012.
Brand names
Escitalopram is sold under the following brand names:
- Animaxen (Colombia)
- Anxiset-E (India)
- Cipralex
- Escital (Nigeria)
- Citalin
- Citram (Croatia)
- Ecytara (Slovenia)
- Elicea
- Entact (Greece)
- Escitalopram Actavis (Finland)
- Escitil (Czech Republic)
- Esitalo (Australia)
- Esopram, by Actavis (Iceland)
- Esto (Israel)
- Escitalopram Teva (Israel)
- Exodus (Brazil)
- Lexam
- Lexamil (South Africa)
- Lexapro
- Losita (Bangladesh)
- Nexito
- Reposil (Chile)
- Selectra (Russia)
- Selpram (Pakistan)
- Seroplex
- Sipralexa (Belgium)
References
- ^ a b c NHS pays millions of pounds more than it needs to for drugs, The Independent. Retrieved 05/10/2011.
- ^ “Escitalopram Oxalate”. The American Society of Health-System Pharmacists. Retrieved 3 April 2011.
- ^ Kasper, S; Stein, DJ; Loft, H; Nil, R (2005). “Escitalopram in the treatment of social anxiety disorder: Randomised, placebo-controlled, flexible-dosage study”. The British journal of psychiatry : the journal of mental science 186 (3): 222–6.doi:10.1192/bjp.186.3.222. PMID 15738503.
- ^ Stahl, SM; Gergel, I; Li, D (2003). “Escitalopram in the treatment of panic disorder: A randomized, double-blind, placebo-controlled trial”. The Journal of clinical psychiatry 64(11): 1322–7. PMID 14658946.
- ^ Stein, DJ; Andersen, EW; Tonnoir, B; Fineberg, N (2007). “Escitalopram in obsessive-compulsive disorder: A randomized, placebo-controlled, paroxetine-referenced, fixed-dose, 24-week study”. Current medical research and opinion 23 (4): 701–11. doi:10.1185/030079907X178838. PMID 17407626.
- ^ a b Cipriani, A; Santilli C; Furukawa TA; Signoretti A; Nakagawa A; McGuire H; Churchill R; Barbui C (2009 April 15). “Escitalopram versus other antidepressant agents for depression”. In Cipriani, Andrea. Cochrane database of systematic reviews(2): CD006532. doi:10.1002/14651858.CD006532.pub2. PMID 19370639. CD006532.
- ^ Cipriani, A; Furukawa TA; Salanti G; Geddes JR; Higgins JP; Churchill R; Watanabe N; Nakagawa A; Omori IM; McGuire H; Tansella M; Barbui C (2009 February 28). “Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis”. Lancet 373 (9665): 746–58. doi:10.1016/S0140-6736(09)60046-5. PMID 19185342.
- ^ Ioannidis JP (2008). “Effectiveness of antidepressants: an evidence myth constructed from a thousand randomized trials?”. Philos Ethics Humanit Med 3: 14.doi:10.1186/1747-5341-3-14. PMC 2412901. PMID 18505564.
- ^ Fournier JC, DeRubeis RJ, Hollon SD, Dimidjian S, Amsterdam JD, Shelton RC, Fawcett J (January 2010). “Antidepressant drug effects and depression severity: a patient-level meta-analysis”. JAMA 303 (1): 47–53. doi:10.1001/jama.2009.1943.PMID 20051569.
- ^ Ou, JJ; Xun, GL; Wu, RR; Li, LH; Fang, MS; Zhang, HG; Xie, SP; Shi, JG; Du, B; Yuan, XQ; Zhao, JP (2011 Feb). “Efficacy and safety of escitalopram versus citalopram in major depressive disorder: a 6-week, multicenter, randomized, double-blind, flexible-dose study.”. Psychopharmacology 213 (2-3): 639–46. doi:10.1007/s00213-010-1822-y. PMID 20340011.
|accessdate=requires|url=(help) - ^ Yevtushenko, VY; Belous, AI; Yevtushenko, YG; Gusinin, SE; Buzik, OJ; Agibalova, TV (2007 Nov). “Efficacy and tolerability of escitalopram versus citalopram in major depressive disorder: a 6-week, multicenter, prospective, randomized, double-blind, active-controlled study in adult outpatients.”. Clinical therapeutics 29 (11): 2319–32.PMID 18158074.
- ^ Colonna, L; Andersen, HF; Reines, EH (2005 Oct). “A randomized, double-blind, 24-week study of escitalopram (10 mg/day) versus citalopram (20 mg/day) in primary care patients with major depressive disorder.”. Current medical research and opinion 21(10): 1659–68. PMID 16238906.
- ^ Moore, N; Verdoux, H; Fantino, B (2005 May). “Prospective, multicentre, randomized, double-blind study of the efficacy of escitalopram versus citalopram in outpatient treatment of major depressive disorder.”. International clinical psychopharmacology 20 (3): 131–7. PMID 15812262.
- ^ Montgomery, Stuart; Hansen, Thomas; Kasper, Siegfried (28 September 2010). “Efficacy of escitalopram compared to citalopram: a meta-analysis”. The International Journal of Neuropsychopharmacology 14 (02): 261–268.doi:10.1017/S146114571000115X. PMID 20875220.
- ^ Gorman, JM; Korotzer, A; Su, G (2002 Apr). “Efficacy comparison of escitalopram and citalopram in the treatment of major depressive disorder: pooled analysis of placebo-controlled trials.”. CNS spectrums 7 (4 Suppl 1): 40–4. PMID 15131492.
- ^ Trkulja, V (2010 Feb). “Is escitalopram really relevantly superior to citalopram in treatment of major depressive disorder? A meta-analysis of head-to-head randomized trials.”. Croatian medical journal 51 (1): 61–73. PMID 20162747.
- ^ “Citalopram and escitalopram: QT interval prolongation—new maximum daily dose restrictions (including in elderly patients), contraindications, and warnings”.Medicines and Healthcare products Regulatory Agency. December 2011. Retrieved March 5, 2013.
- ^ Van Gorp, Freek; Whyte, Ian M.; Isbister, Geoffrey K. (2009). “Clinical and ECG Effects of Escitalopram Overdose”. Annals of Emergency Medicine 54 (3): 404–8.doi:10.1016/j.annemergmed.2009.04.016. PMID 19556032.
- ^ FDA Center for Drug Evaluation and Research (2001). “Review and evaluation of clinical data for application 21-323″. Retrieved 2009-12-03.
- ^ Bolton JM, Sareen J, Reiss JP (2006). “Genital anesthesia persisting six years after sertraline discontinuation”. J Sex Marital Ther 32 (4): 327–30.doi:10.1080/00926230600666410. PMID 16709553.
- ^ Clayton A, Keller A, McGarvey EL (2006). “Burden of phase-specific sexual dysfunction with SSRIs”. Journal of Affective Disorders 91 (1): 27–32.doi:10.1016/j.jad.2005.12.007. PMID 16430968.
- ^ Lexapro prescribing information
- ^ Csoka AB, Bahrick AS, Mehtonen O-P (2008). “Persistent Sexual Dysfunction after Discontinuation of Selective Serotonin Reuptake Inhibitors (SSRIs)”. J Sex Med. 5 (1): 227–33. doi:10.1111/j.1743-6109.2007.00630.x. PMID 18173768.
- ^ Baldwin DS, Reines EH, Guiton C, Weiller E (2007). “Escitalopram therapy for major depression and anxiety disorders”. Ann Pharmacother 41 (10): 1583–92.doi:10.1345/aph.1K089. PMID 17848424.
- ^ Pigott TA, Prakash A, Arnold LM, Aaronson ST, Mallinckrodt CH, Wohlreich MM (2007). “Duloxetine versus escitalopram and placebo: an 8-month, double-blind trial in patients with major depressive disorder”. Curr Med Res Opin 23 (6): 1303–18.doi:10.1185/030079907X188107. PMID 17559729.
- ^ Davidson JR, Bose A, Wang Q (2005). “Safety and efficacy of escitalopram in the long-term treatment of generalized anxiety disorder”. J Clin Psychiatry 66 (11): 1441–6.doi:10.4088/JCP.v66n1115. PMID 16420082.
- ^ Kasper S, Lemming OM, de Swart H (2006). “Escitalopram in the long-term treatment of major depressive disorder in elderly patients”. Neuropsychobiology 54 (3): 152–9. doi:10.1159/000098650. PMID 17230032.
- ^ Guerdjikova, AI; McElroy SL, Kotwal R, et al. (January 2008). “High-dose escitalopram in the treatment of binge-eating disorder with obesity: a placebo-controlled monotherapy trial”. Human Psychopharmacology: Clinical and Experimental23 (1): 1–11. doi:10.1002/hup.899. PMID 18058852.
- ^ Levenson M, Holland C. “Antidepressants and Suicidality in Adults: Statistical Evaluation. (Presentation at Psychopharmacologic Drugs Advisory Committee; December 13, 2006)”. Retrieved 2007-05-13.
- ^ Stone MB, Jones ML (2006-11-17). “Clinical Review: Relationship Between Antidepressant Drugs and Suicidality in Adults” (PDF). Overview for December 13 Meeting of Pharmacological Drugs Advisory Committee (PDAC). FDA. pp. 11–74. Retrieved 2007-09-22.
- ^ Levenson M; Holland C (2006-11-17). “Statistical Evaluation of Suicidality in Adults Treated with Antidepressants” (PDF). Overview for December 13 Meeting of Pharmacological Drugs Advisory Committee (PDAC). FDA. pp. 75–140. Retrieved 2007-09-22.
- ^ Gunnell D, Saperia J, Ashby D (2005). “Selective serotonin reuptake inhibitors (SSRIs) and suicide in adults: meta-analysis of drug company data from placebo controlled, randomized controlled trials submitted to the MHRA’s safety review”. BMJ330 (7488): 385. doi:10.1136/bmj.330.7488.385. PMC 549105. PMID 15718537.
- ^ Khan A, Schwartz K (2007). “Suicide risk and symptom reduction in patients assigned to placebo in duloxetine and escitalopram clinical trials: analysis of the FDA summary basis of approval reports”. Ann Clin Psychiatry 19 (1): 31–6.doi:10.1080/10401230601163550. PMID 17453659.
- ^ Budur, Kumar; Hutzler, Jeffrey (June 2004). “Severe suicidal ideation with escitalopram (Lexapro): a case report”. Primary Care Psychiatry 9 (2): 67–68.doi:10.1185/135525704125004222.
- ^ Karch, Amy (2006). 2006 Lippincott’s Nursing Drug Guide. Philadelphia, Baltimore, New York, London, Buenos Aires, Hong Kong, Sydney, Tokyo: Lippincott Williams & Wilkins. ISBN 1-58255-436-6.
- ^ Malling, D.; Poulsen, M.; Søgaard, B. (2005). “The effect of cimetidine or omeprazole on the pharmacokinetics of escitalopram in healthy subjects”. British Journal of Clinical Pharmacology 60 (3): 287–290. doi:10.1111/j.1365-2125.2005.02423.x.PMC 1884771. PMID 16120067. edit
- ^ “Lexapro – Warnings”. RxList. 12/08/2004. Retrieved 2006-10-22.
- ^ Alwan S, Reefhuis J, Rasmussen SA, Olney RS, Friedman JM, for the National Birth Defects Prevention Study. Use of selective serotonin-reuptake inhibitors in pregnancy and the risk of birth defects. N Engl J Med 2007;356:2684–92.
- ^ van Gorp F, Whyte IM, Isbister GK. Clinical and ECG effects of escitalopram overdose. Ann. Emer. Med. 54: 404-408, 2009.
- ^ Haupt D. Determination of citalopram enantiomers in human plasma by liquid chromatographic separation on a Chiral-AGP column. J. Chrom. B 685: 299-305, 1996.
- ^ R. Baselt, Disposition of Toxic Drugs and Chemicals in Man, 8th edition, Biomedical Publications, Foster City, CA, 2008, pp. 552-553.
- ^ For an overview of supporting data, see Sánchez C, Bøgesø KP, Ebert B, Reines EH, Braestrup C (2004). “Escitalopram versus citalopram: the surprising role of the R-enantiomer”. Psychopharmacology (Berl.) 174 (2): 163–76. doi:10.1007/s00213-004-1865-z. PMID 15160261.
- ^ Chen F, Larsen MB, Sánchez C, Wiborg O (2005). “The (S)-enantiomer of (R,S)-citalopram, increases inhibitor binding to the human serotonin transporter by an allosteric mechanism. Comparison with other serotonin transporter inhibitors”.European Neuropsychopharmacology 15 (2): 193–198.doi:10.1016/j.euroneuro.2004.08.008. PMID 15695064.
- ^ Mansari ME, Wiborg O, Mnie-Filali O, Benturquia N, Sánchez C, Haddjeri N (2007). “Allosteric modulation of the effect of escitalopram, paroxetine and fluoxetine: in-vitro and in-vivo studies”. The International Journal of Neuropsychopharmacology 10 (1): 31–40. doi:10.1017/S1461145705006462. PMID 16448580.
- ^ “2000 Annual Report. p 28 and 33″ (PDF). Lundbeck. 2000. Retrieved 2007-04-07.
- ^ “”New drugs from old”. Presented at the Medical Journal Club, Morriston Hospital, by Scott Pegler, pharmacist at the National Health Service, UK, on November 20, 2006.” (PPT). Retrieved 2007-04-07.
- ^ “New drugs from old”. Drug and Therapeutics Bulletin (BMJ Publishing Group Ltd.)44 (10): 73–77. 2006. doi:10.1136/dtb.2006.441073. PMID 17067118.
- ^ Miranda Hitti. “FDA OKs Generic Depression Drug – Generic Version of Lexapro Gets Green Light”. WebMD. Retrieved 2007-10-10.
- ^ Marie-Eve Laforte (2006-07-14). “US court upholds Lexapro patent”. FirstWord. Retrieved 2007-10-10.
- ^ “Forest Laboratories Receives Patent Term Extension for Lexapro” (Press release). PRNewswire-FirstCall. 2006-03-02. Retrieved 2009-01-19.
- ^ Harris, “A Drug Maker’s Playbook Reveals a Marketing Strategy”
- ^ Lexapro Fiscal 2004 Marketing Plan
- ^ “Forest Laboratories: A Tale of Two Whistleblowers” article by Alison Frankel inThe American Lawyer February 27, 2009
- ^ United States of America v. Forest Laboratories Full text of the federal complaint filed in the US District Court for the district of Massachusetts
- ^ “Drug Maker Is Accused of Fraud” article by Barry Meier and Benedict Carey inThe New York Times February 25, 2009
- ^ “Forest Laboratories, Inc. Provides Statement in Response to Complaint Filed by U.S. Government” Forest press-release. February 26, 2009.
- “A Drug Maker’s Playbook Reveals a Marketing Strategy” article in The New York Times by Gardiner Harris, September 1, 2009
- Royal Pharmaceutical Society of Great Britain (September 2009). British National Formulary (BNF 58). UK: BMJ Group and RPS Publishing. ISBN 978-0-85369-778-7.
- U.S. National Library of Medicine: Drug Information Portal — Escitalopram
- Lexapro (Forest Laboratories) Official Lexapro homepage
- Cipralex (Lundbeck) Official Cipralex homepage
- Pharmacological information Lexapro
- Cipla Medpro Official Cipla Medpro homepage






Subscribe to:
Posts (Atom)